
[Editorial note: The following presentation, A Review of the JFK Cranial x-Rays and Photographs, was prepared and delivered by neurologist, Dr. Michael Chesser, at the 2015 JFK Lancer Conference in Dallas, Texas. His work also supports the findings of Dr. David Mantik. According to Dr. Chesser:
“I viewed the original autopsy skull X-rays at the archives this year [2015] and I confirmed [Mantik’s] optical density readings of the lateral skull film, which support his conclusion that there was manipulation. Hopefully there will come a time when better copies of the autopsy x-rays and photographs will be made available for review by a wider audience and the evidence will speak for itself. I applaud Dr. David Mantik for his courage in reporting the truth.”
While there are many debatable items of evidence in this case, many of which cannot be proved one way or another, the medical evidence has now been subjected to scrutiny by several eminently qualified medical experts and a physicist. Dr. Michael Chesser demonstrates, among other things, that these rather disturbing findings are replicable. We thank him for his good work and dedication to the truth. — Greg Burnham]
- Please voice your opinion by taking the poll at the end of this article.
A Review of the JFK Cranial x-Rays and Photographs
by Dr. Michael Chesser
This review of the JFK cranial x-rays and photographs is based upon two visits to the archives in College Park, and also a visit to the Presidential Library in Boston. I hope that I can do justice to the evidence, and I’ll do my best to describe these x-rays and photographs. Before we start, I just want to say that I regret that we have to continue to show these photographs, which show the violence and trauma inflicted upon President Kennedy. Unfortunately there is no other way to get to the truth of what actually happened that day. I apologize to the Kennedy family for this.

I’m fascinated with the different ways that people are brought into this journey – to find the truth – and I’d like to tell you a little bit about my journey. I was 8 years old in November of 1963, and I vividly remember that day and the next 3 days, and I remember the grief of my parents and teachers. I remember watching the funeral and the procession to Arlington cemetery – and I remember the heaviness that settled over everyone. I was oblivious to the House Select committee investigation – too busy in med school – and then of course I watched Oliver Stone’s JFK, and read a couple of books over the next year – but I can’t even tell you which books I read. Then two years ago I read James Douglass’ book, and that struck a chord in me –it lit a fire under me – and I’ve been trying to catch up ever since.
In Sept 2014 I saw the notice about the AARC 50th anniversary of the Warren Commission conference, and I decided to go. Many of the people that I met at the conference encouraged me to go to the archives. I didn’t realize that so few had actually seen the original x-rays and photos, and approval to view these materials is difficult to obtain. Eventually I was approved to view the cranial x-rays only – based upon my qualifications as a neurologist. Other than my 28 years experience as a neurologist, my background includes 2 years as a primary care navy medical officer. I also worked my way through the second year of med school as a morgue assistant – and I assisted on multiple autopsies during that year. I’ve been reviewing skull x-rays since medical school – so I felt qualified – but I have to say that there are thousands of people who are qualified to review these films.
I visited the archives before I really knew much about the medical evidence – before reading David Lifton, Doug Horne, Sherry Fiester, Gary Aguilar, and others. I had read some of David Mantik’s writings, but not all of them. It would have been useful to have a better background of knowledge of the autopsy, however I believe that I viewed these films with an open mind, and with a healthy scientific curiosity.
Many of you recognize the national archives II building in College Park. The autopsy materials were turned over to the archives in 1965 – it was mandated by public law 89-318, passed by congress in Nov 1965, that these materials were placed in the custody of the federal government – up to that point they were kept by Robert Kennedy. At the time they were turned over, a deed of gift was set up, to review requests to view the autopsy materials.
A Review of the JFK Cranial x-Rays and Photographs
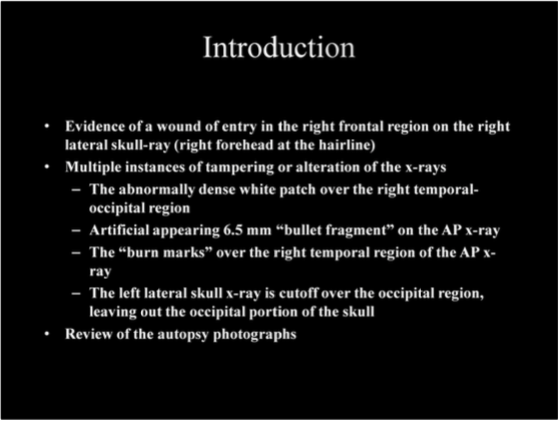
This is what we’re going to talk about – in a nutshell – I’m going to tell you why I believe that there is in fact, evidence, of a shot from the front, with entry in the upper right forehead. I agree with Dr. David Mantik that there are multiple instances of manipulation or tampering of the evidence, and I would like to add the so called burn marks to this collection. And we will review some of the photographs – especially the scalp retraction photograph.
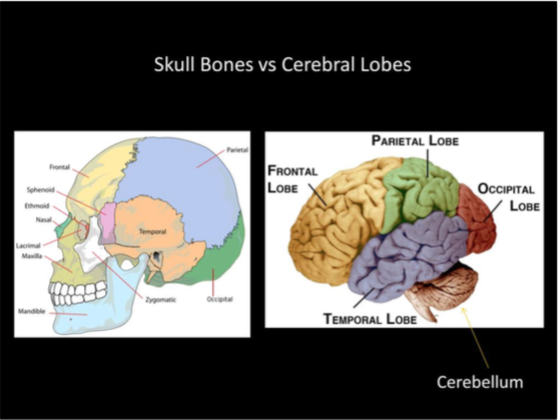
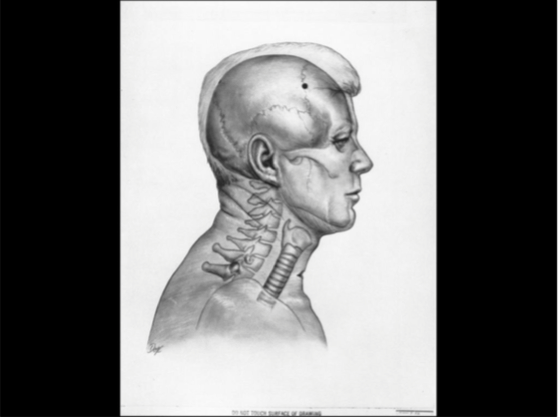
When we talk about the skull bones and the lobes of the brain, we use the same terms, however their territories don’t exactly match. As you see here, the largest skull bone is the parietal bone, and it covers multiple lobes of the brain. The cerebellum is covered primarily by the occipital bone. As you see there is a marked difference in appearance of the cerebellum compared with the cerebrum – when I heard that many of the doctors at Parkland saw cerebellar tissue in the wound, and actually falling out of the skull defect, I knew that something wasn’t right with the official version of the wounds. The delicate folia of the cerebellum are so much different than the lobular gyrus pattern of the cerebral hemispheres – well I just can’t imagine that many medical professionals mistaking the two. Only recently did I read Gary Aguilar’s essay of the various description of the wounds made by medical personnel at Parkland and Bethesda, and most of the observers described a skull defect of the occipital region.
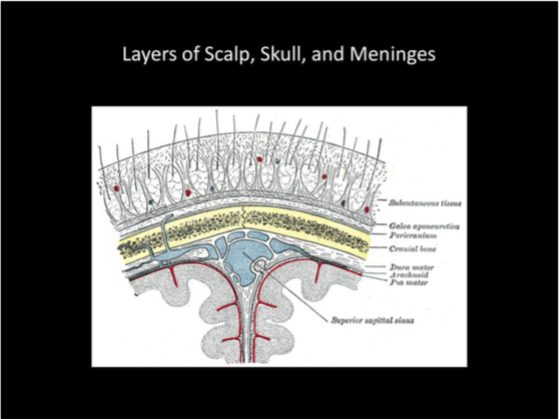
This is to show the layers of tissue between the scalp and the brain – the scalp tissue has a very thick, tough base layer called the galea aponeurotica – and we’ll come back to that later. The skull bone itself has a covering called periosteum, and then inside the skull the brain is surrounded by three layers of the meninges. Radiation passing through the skull to the x ray film passes through all of these tissues, as well as blood vessels and spinal fluid, and they all contribute to the image we see on the film.
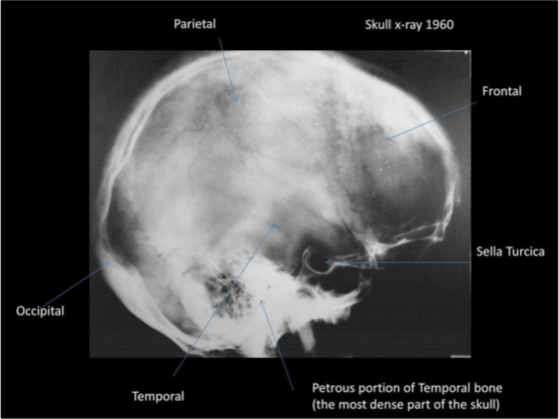
This lateral skull x-ray was performed on President Kennedy in 1960, and it took me a while, but I located the original at the Presidential Library in Boston, where it was labeled as a sinus x-ray. This is shown here to show that the petrous portion of the temporal bone is the most dense, and brightest, region on a skull x-ray. The pattern of variable density throughout the skull is typical. The autopsy x-rays show an abnormally dense and homogeneous appearance in the occipital region of the skull. I viewed this original x-ray at the JFK Library in Boston on 7/23/15 and measured the optical density of various areas of the film, for comparison with the autopsy x-rays. The pituitary gland sits in the sella turcica — and the sella turcica appears relatively enlarged compared with the overall skull dimensions on this skull x-ray.
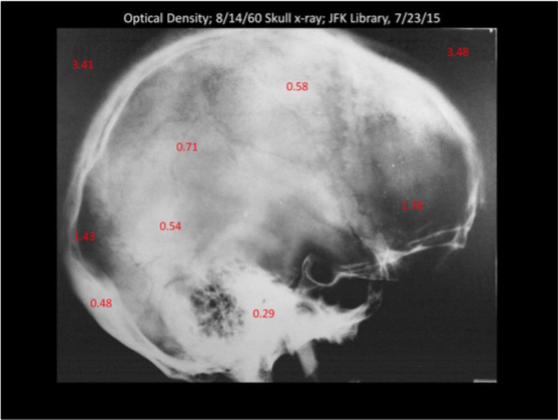
These OD readings were taken with an X-Rite 341 portable optical densitometer. Calibration was performed. This shows that the most dense part of the skull is easily the petrous (latin “petrosus” – stone hard) portion of the temporal bone. This also shows that the optical densitometer can demonstrate differences in density which aren’t apparent to the human eye.
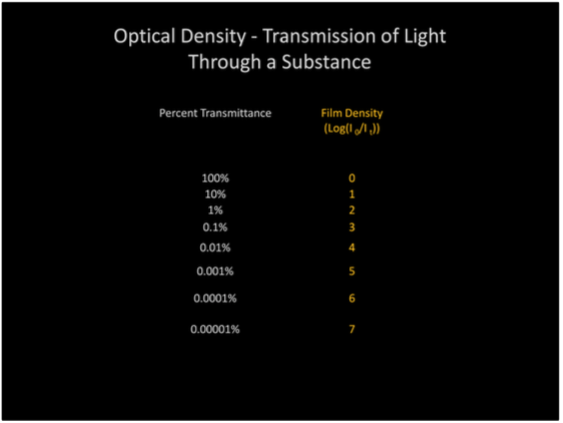
The optical density measurement is a logarithmic value, as shown, with a density of 1 for 10% of the light transmitted through the film, and a density of 2 is equivalent to 1 % of light transmission through the film. Optical density readings were used for quality control of x-ray film. A lower optical density measurement indicates a more dense region of the skull.
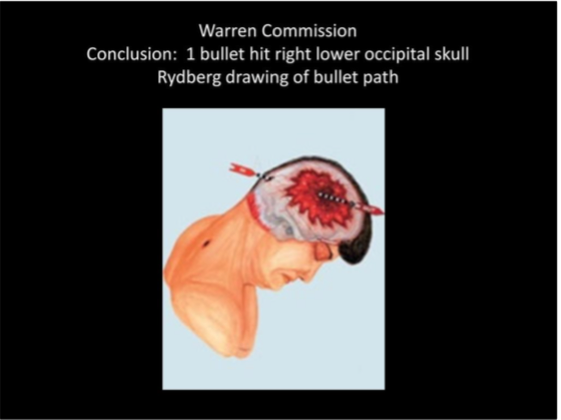
The Bethesda pathologists reported an entry wound low in the right occiput – lateral to the protuberance. This illustration was made for the Warren Commission, based upon the pathologist’s description. The x-rays and photographs that we are reviewing today were not officially examined by the Warren Commission.

Compare the angle of President Kennedy’s head on the previous illustration with the appearance on the Zapruder film. His head was turned to the left and tilted forward at the time of a shot to the head in frame 313.
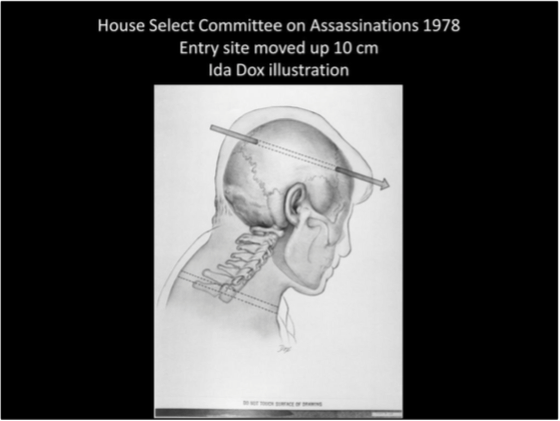
The Clark panel in 1968 and also the HSCA physicians moved the wound of entry up about 10 cm to the posterior parietal area, and the exit at the right coronal suture line. The autopsy pathologists disagreed with this change of entry location. I think that one of the primary reasons that the entry location was changed was because of the appearance of the x-rays, and because the time was approaching for the autopsy x-rays to be made available for viewing to other physicians.
Again, an illustration by “Ida Dox”(pseudonym).
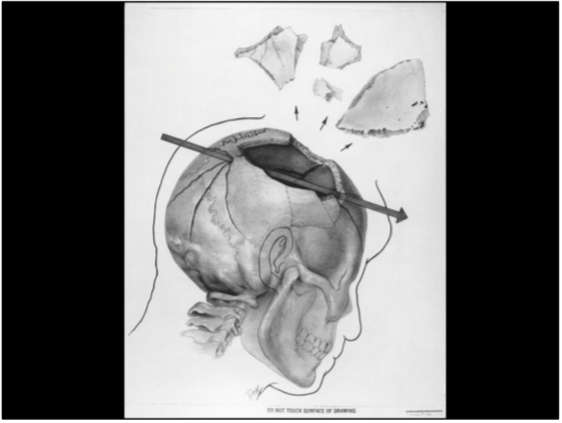
And again, the exit location according to the HSCA, at the coronal suture.
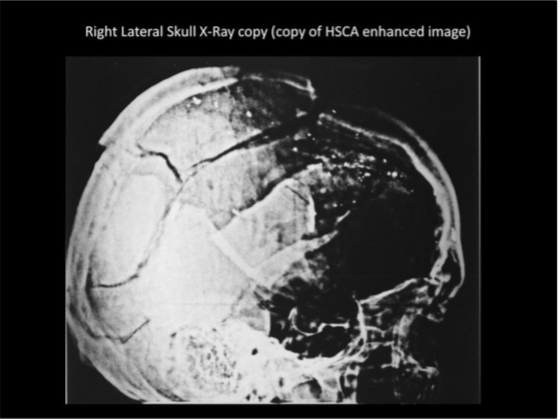
Dr. G. M. McDonnel oversaw the production of computer enhanced copies of the original skull x-rays for the HSCA, and then copies of these copies were made available and released by NARA. Dr. McDonnel’s interesting past and his interpretation of these x-rays will be discussed later.
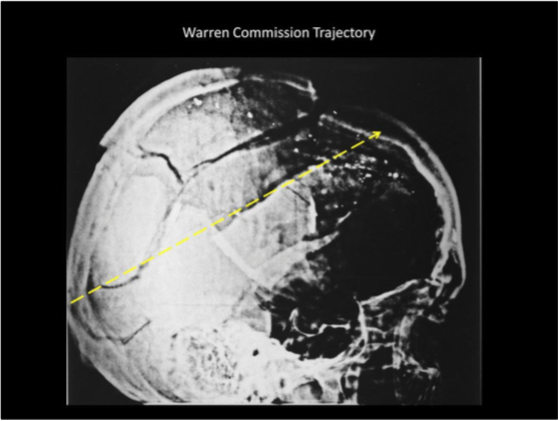
I think that one of the reasons that they moved the entry wound up was due to the fragment particle trail shown in the right lateral skull x-ray. If a line is drawn from the Warren Commission entry site and the proposed exit site, you’ll notice that the particle trail doesn’t correspond with these sites. The prominent particle trail is located in the upper portion of the skull.
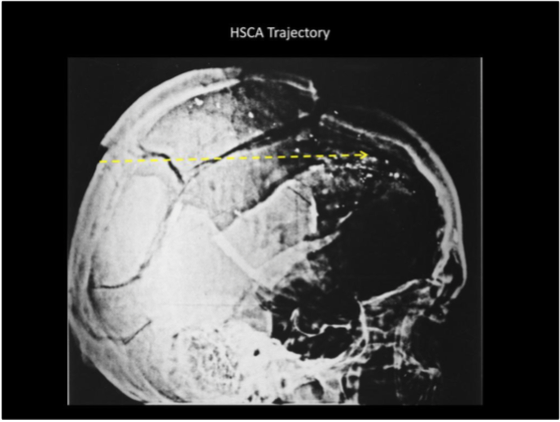
Now if you do the same for the HSCA entry and exit sites, you’ll notice that the line is closer to the particle trail, but it still doesn’t seem to correspond.
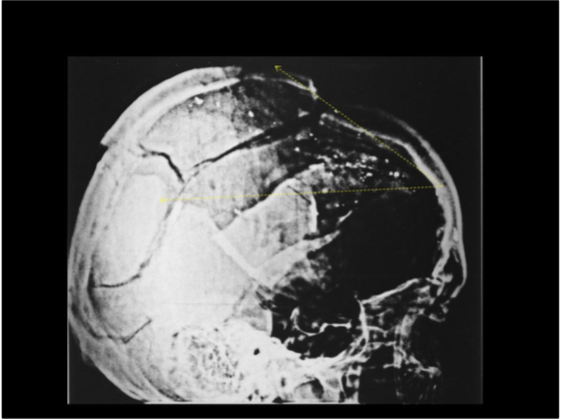
I am just one of many who believe that the entry site responsible for this particle trail was in the right frontal region, at or just above the hairline. If you notice the location, I’ve moved it up slightly from the skull defect which I think represents the entry site, because the right side of the frontal bone had separated and had dropped in relation to the left frontal skull.

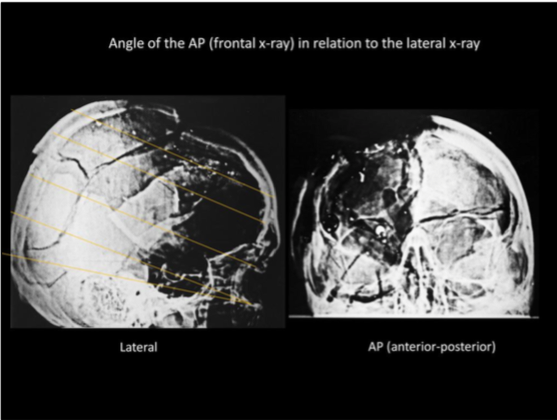
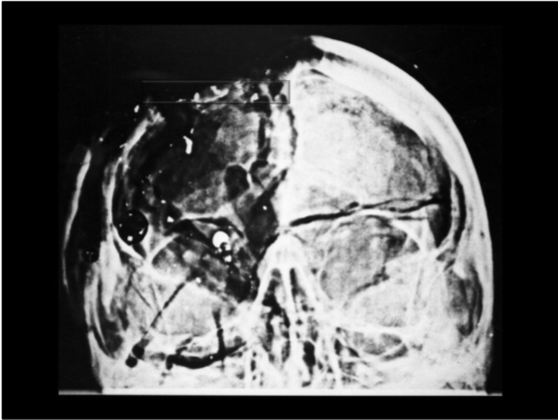
On the frontal view, the AP x-ray, the particle trail is located high in this image, which is probably in the scalp and meninges. There is a lot going on in this image, with multiple skull fractures, and much of the skull missing over the right frontal, parietal, occipital regions. The orbital rim is fractured on both sides. The vomer bone (nasal) is fractured. You can see that there is brain shadow on the left side, but you really can’t see any on the right side. The burn marks are located on the right side, lateral to the orbital wall. There is low density, or missing bone behind the nasal bones and at the lower edge of the left orbit – and I agree with Dr. Mantik that this suggests missing occipital bone, extending over to the left side.
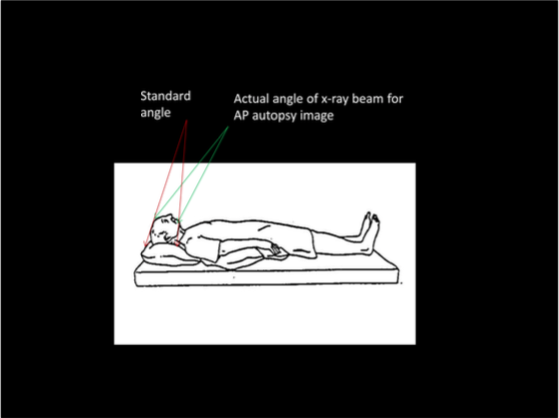
The standard angle of the x-ray beam for an AP skull x-ray is shown on the in red, and the approximate angle from the autopsy AP skull x-ray is shown on the right, in green. If the angle is correct, the lower edge of the orbital rim lines up with the external auditory canal, in the petrous bone.
I did a rough calculation of the AP film angle and arrived at 13 degrees above a line from the lower orbital rim to the petrous apex. I think others have measured this around 15 to 16 degrees. One problem when you’re looking at the lateral skull x-ray copies is that the orbital rim isn’t clearly visible – this was blacked out when they obscured the facial bones in this copy.
This angle then allows you to determine the location of objects in 3 dimensions, when combined with the lateral image.
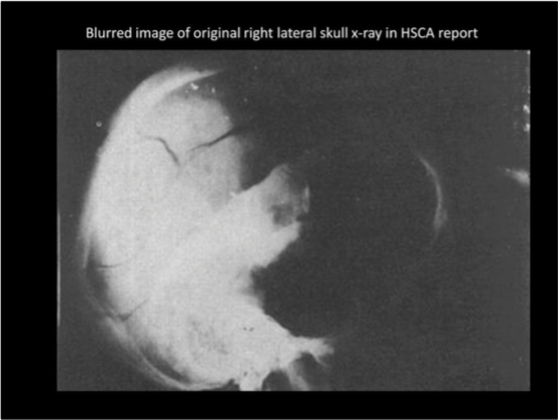
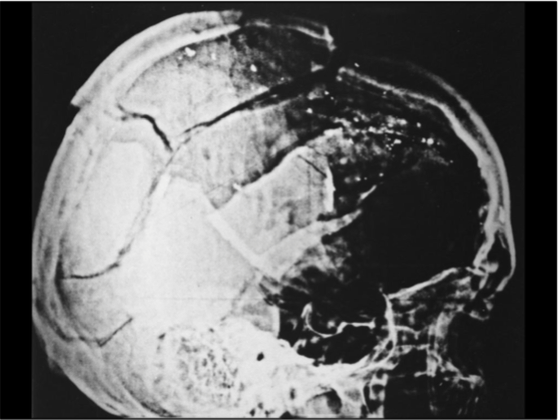
In the HSCA report you’ll find this very blurred image of the original right lateral skull x-ray (actually the inventory lists two left lateral skull x-rays). Looking at this image in the report would make you think that this x-ray is in horrible condition, and that the anterior half of the skull was so dim that no useful information could be obtained. That couldn’t be further from the truth. The actual original x-rays are in excellent condition, showing only minor aging, and this blurred copy doesn’t represent the original film well. This blurred image is very misleading – the purported reason for the need to enhance the x-rays was the poor image quality – that simply isn’t true.
This is from the image we just saw, now focusing on the frontal bone.
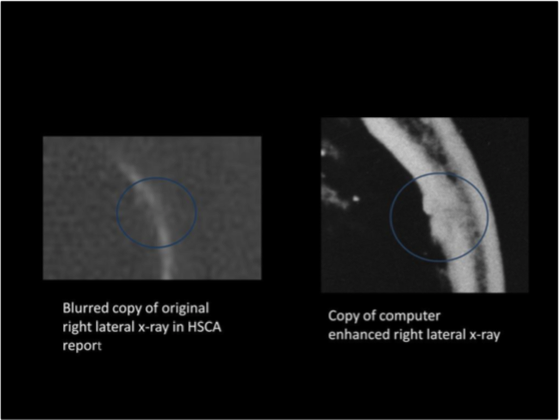
Again, on the left, the blurred image from the HSCA report, from the original x-ray, and on the right, this same area from a copy of the computer enhanced right lateral x-ray. Notice that the gap in the bone on the left, now appears solid. The next question is –what are the two bulging, dense areas projecting on the inner side of the right frontal bone on the copy.

A Review of the JFK Cranial x-Rays and Photographs
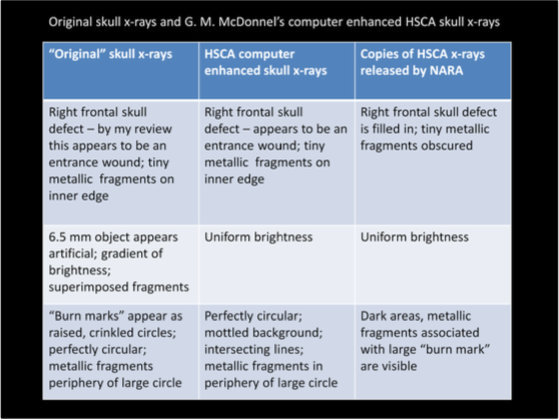
This is what I saw on the original right lateral skull x-ray at the archives. There is a gap in the bone – not very big, maybe 3 mm, but remember that this is a composite of all the material between the x-ray machine and the film – when viewed from the side, a hole in the frontal bone may not be seen at all, and if it is, it won’t appear as wide as it’s actual width. I think that this defect is probably due to a combination of an entry wound and associated radial fracture line(s). The most important finding here is the proximity of these tiny metallic fragments to this bone defect. This location, on the intracranial side of the bony defect, is highly suggestive of an entry wound. One of the principles of skull ballistics is that the largest fragments travel the furthest from the entry site, with the smallest traveling the least distance, and that is exactly what is seen on this right lateral skull x-ray. Tiny fragments are seen were seen on the inner side of this right frontal skull defect, and the largest fragments were noted in the back of the skull.
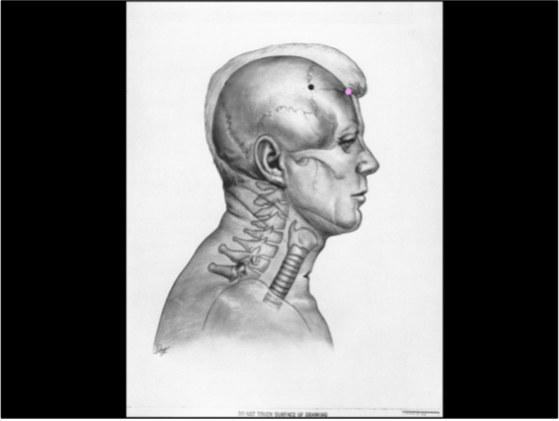
The approximate location is seen in pink here, in relation to the skull and facial profile of the President, at the hairline.

I believe that this location also corresponds to the area circled here.

And again, this same area appears differently in this autopsy photograph – in this image, the area appears to be obscured by a fuzzy dark blob – it appeared this way on the actual photograph at the archives – I believe that this photo has been altered.
Now, going back to the AP skull x-ray, the obvious question is – where does this map out? I believe that it is at the level noted in this image, lined up with the main part of the fragment particle trail, based upon the angle at which the AP x-ray was made. Why are we not able to see the frontal bone at this level? There are different possible explanations – first there may not be enough tissue, at this level, to show up on the AP x-ray. If there isn’t any significant amount of brain tissue behind the frontal bone, and the parietal bone is missing behind it, it may not be dense enough to show up on the image.
Another possibility, that seems improbable, but in this case I think that you have to look at all possibilities, is that this piece of frontal bone, which was mobile and not connected to surrounding skull, was simply removed for the x-ray. We know that the pathologists and morticians had to reconstruct the skull, and the right forehead appeared sunken, the right eye was bulging out. The corpsmen describe the pathologists actually positioning portions of the frontal bone back into place.
I favor the first explanation. And I also think that if present day technology could be used to make good digital copies of the original x-rays, that the images could then be analyzed and we could obtain much more information and we could possibly identify the entrance wound on this AP x-ray.
Without going into detail in this presentation, I would just like to say that I agree with Sherry Fiester’s trajectory analysis and her conclusion that a right frontal entry most likely came from a shot from the area of the triple overpass. This does not exclude a shot being fired from the knoll area, but only suggests that a shot from the knoll was not responsible for this right frontal entry wound.
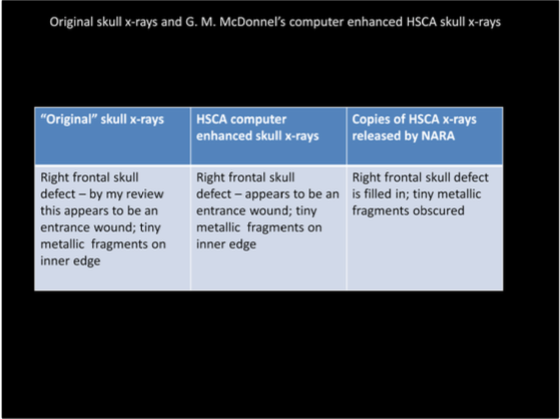
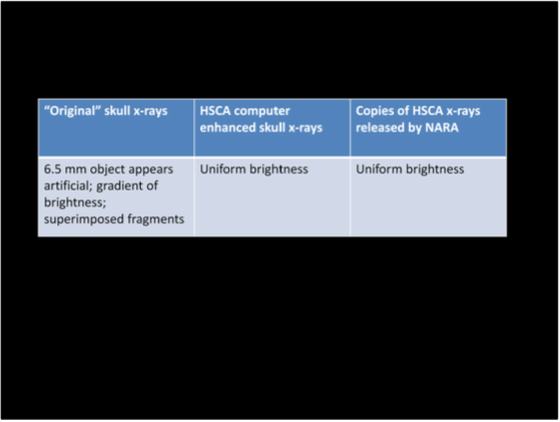
This is a comparison of the original films, the HSCA computer enhanced images, and then the copies of the HSCA images released to the public.
Now I want to go back to the right lateral view, and to focus on the white patch, which Dr. Mantik has written so much about. I agree completely with him, that this points toward tampering.

This is to highlight the “white patch”
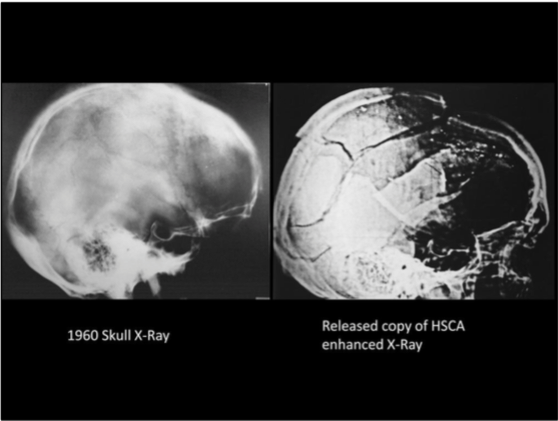
Notice on the left this same area on the 1960 skull x-ray, and how it is much less white, or dense, compared to the base of the skull, the petrous portion of the temporal bone.
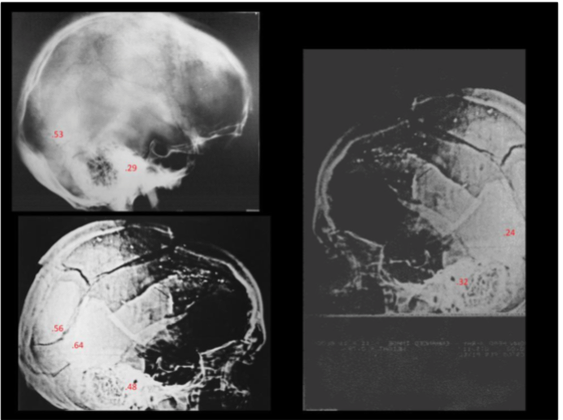
Dr. Mantik took many more optical density readings that I did, but I wanted to show that my readings agree with his – that the white patch appears much more dense than is possible. On the left lateral x-ray, the OD reading was much more dense than the petrous bone – and again, this is not possible. An optical density of .24 is equivalent to a much higher density of the skull in this region, compared with an optical density of .32, and this is not physiologic, even in the face of traumatic alteration of the skull.
Most physicians, myself included, are not aware of the usefulness of optical densitometry for analyzing x-ray film, and I think it was Dr. Mantik’s background as a physicist which caused him to recognize the potential for applying this technology to these films.
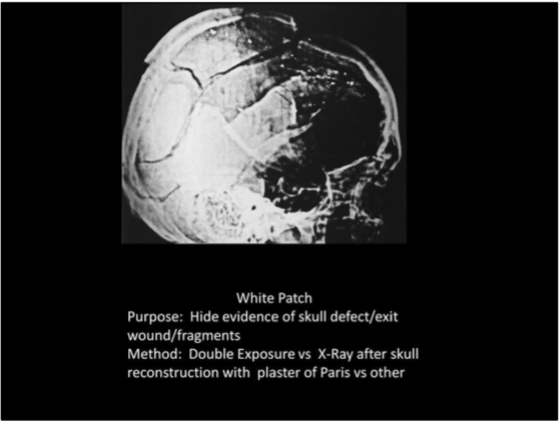
Dr. Mantik has written extensively about the technique of double exposure and how this could have been accomplished with these films. I mention other possibilities because we know that the skull was reconstructed, and that the morticians used a rubber patch combined with plaster of Paris to fill in skull defects after the autopsy. I can’t exclude this, however I think that Dr. Mantik is probably right that double exposure is how the alteration was accomplished.

Puppe’s rule states that a when a fracture line #1 stops at fracture line #2, then fracture line #2 occurred first. The lower circle demonstrates a fracture line ending abruptly at the white patch, rather than intersecting another fracture line.
In the upper circle, fracture line 1 terminates at fracture line 2. According to Puppe’s rule, fracture line 2 occurred first. An entry wound at the HSCA entry site would not be expected to show this pattern.
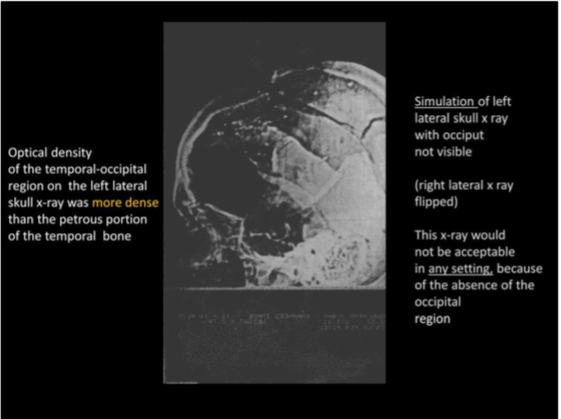
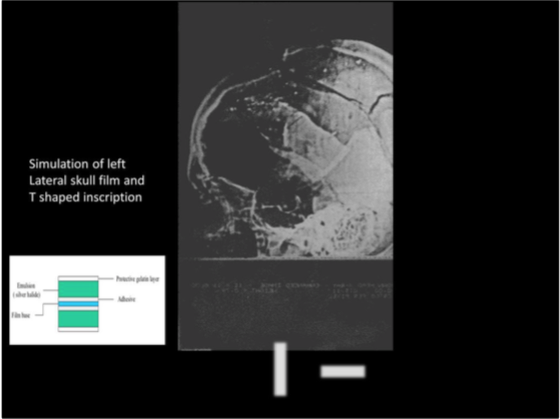
This is a simulation of the left lateral skull x-ray. NARA never released an actual copy of the left lateral skull x-ray. As you see, the back part of the skull isn’t visible. I flipped the image of the right lateral x-ray, and then cut off the occipital region, to simulate the appearance of the left lateral image. I also took optical density measurements of this film, and the left posterior temporal/occipital skull was more dense than the petrous ridge. The skull at the level of the petrous ridge is almost all bone, and it is impossible to explain this finding except to consider that the evidence was altered.
Jerroll Custer stated that the reason the left lateral skull x-ray was cut off at the back was due to the lack of room between the autopsy table and the gallery, and he could not lower the portable x-ray machine low enough to include the entire skull in the image. I asked James Jenkins about this, and he remembered that the portable x-ray machine had a long adjustable arm, and the machine could have been maneuvered to the head of the table, and the arm adjusted to the level to allow adequate imaging of the entire skull. I have difficulty accepting Jerroll Custer’s explanation for this x-ray image, and also his explanation for the burn marks, which will be discussed later.
As I was dictating my impression of the left lateral skull x-ray, and I was surrounded by 3 NARA personnel, I dictated that there appeared to be emulsion overlying the wax mark. Almost immediately one of the NARA personnel left the room and returned with Martha Murphy, and she informed me that a mistake had been made, and I was viewing the HSCA copies of the x-rays. I then asked if I could view the originals, as had been agreed upon, and these were brought out. I don’t believe that I would have viewed the original films without this happening.
Dr. Mantik described emulsion over the T shaped wax mark, which was attributed to Ed Reed marking the film. I agree with him that the surface of the film appeared smooth, when viewed at eye level. The only observation that I had which was different than his is the appearance of this mark when I shone a very bright flashlight over this mark. The mark seemed to light up, distinct from the surrounding area, when I would shine the light across the mark back towards me. I am still not certain what to make of this observation, whether there is wax mark embedded in the external surface of the film or whether it is covered by the film surface, and this is one area that I would like to review again. Nevertheless, in my opinion this is a minor point to consider, in the face of the impossible optical density of the posterior skull on this film, and in view of the cutoff of the occipital skull, where most of the medical personnel describe seeing a skull defect. My review of the scalp retraction photograph also is consistent with a defect in the occipital skull, to be discussed later.
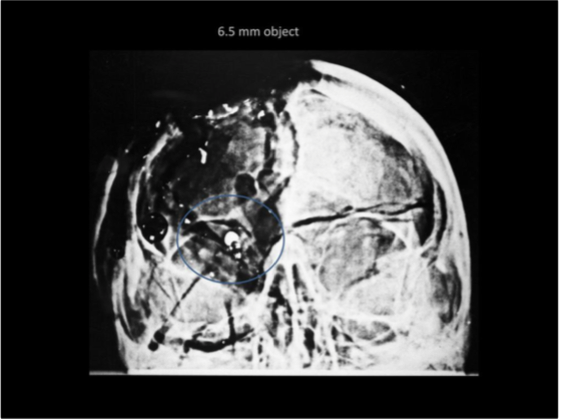
Next, I’d like to talk about the 6.5 mm bright object. The official version is that this is a slice of the midpoint of a Mannlicher Carcano bullet, that broke off and is embedded between the skull and the galea at the HSCA entry wound location.
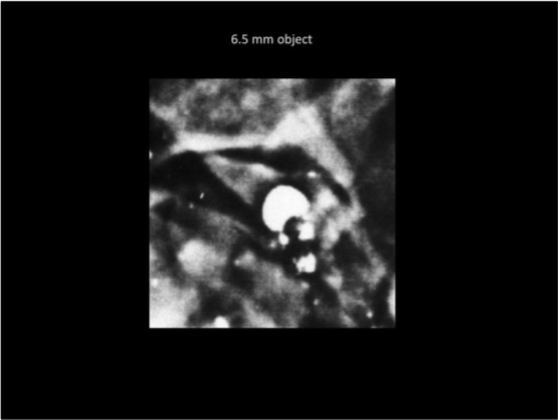
A close up of this object, as seen on the copy of the HSCA computer enhanced image.
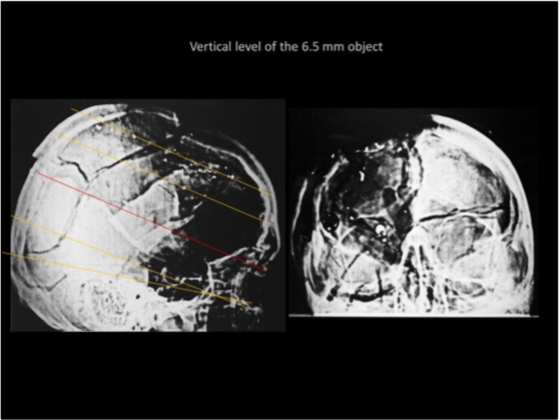
Now where is this 6.5 mm object on the lateral x-ray?
If you take into account the angle taken for the AP x-ray, then it has to lie somewhere along the red line on the left. The only metallic appearing object along this path is the fragment noted at the back of the skull. I agree with Dr. Mantik that this fragment lies within the circumference of the 6.5 mm object, and that the 6.5 mm object was added to the image.
Dr. G.M. McDonnel, who made the computer enhanced images, described this fragment as being located between the outer table of the skull and the galea, the thickest layer of the scalp. He postulated that this broke off when the bullet hit the skull, and this fragment was thrown sideways and away from the skull, embedding itself in this location.
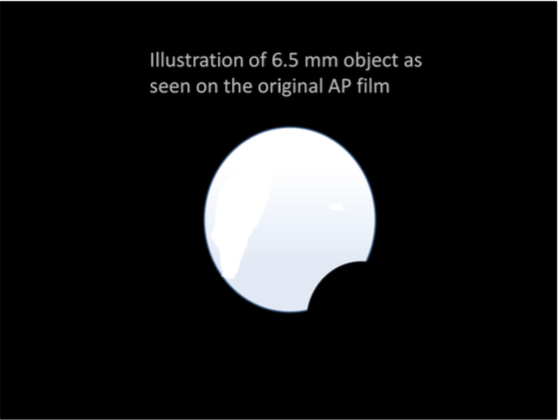
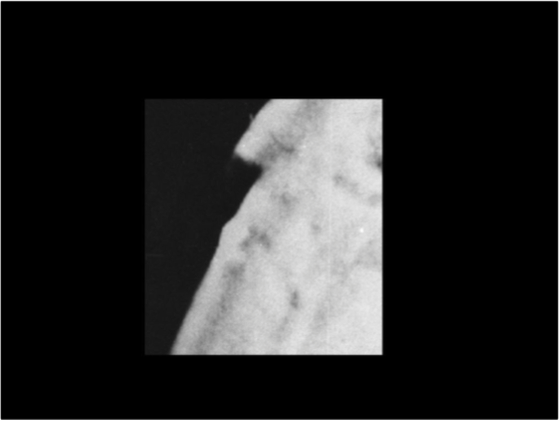
This is how the object appeared to me on the original film. There are two metallic fragments visible within the circumference of this object, and I agree with Dr. Mantik that the largest of these appears to correspond with the object embedded in the galea. I agree with Dr. Mantik’s description of the two fragments visible within the circumference of this object. I saw this only on the original AP x-ray – the HSCA copy shows a uniformly bright object.
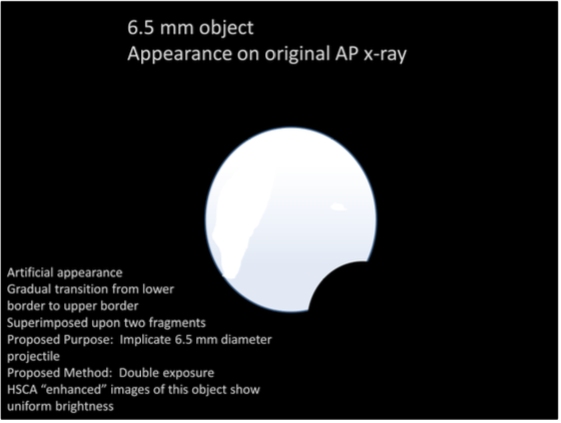
I agree with Dr. Mantik that this is artifactual, and it was most likely added by double exposure. He has described this in detail in his publications.
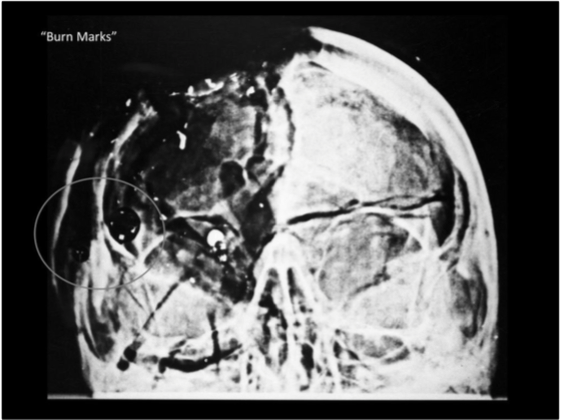
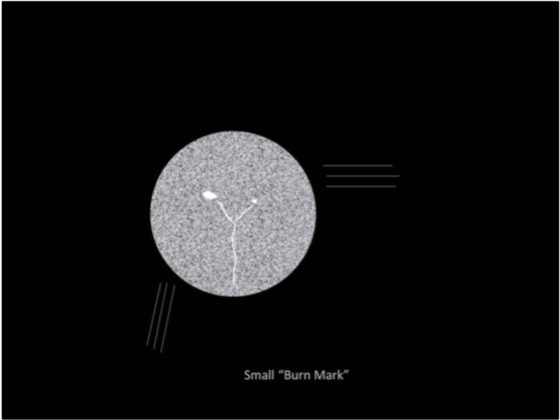
This is the appearance of the “burn marks” on the copy of the computer enhanced image, released by NARA.
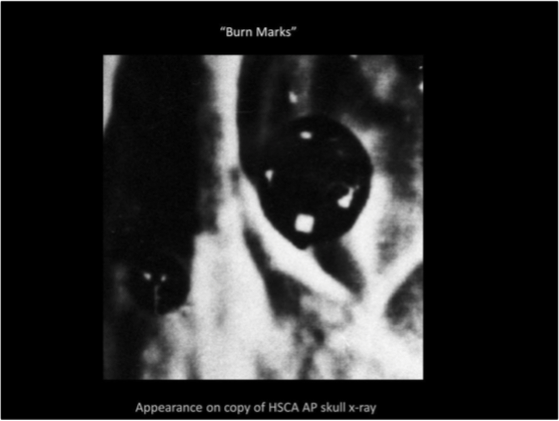
A close up – note that the larger mark is not perfectly round in this copy
Dr. Ebersole took the blame for these marks, and much later Jerroll Custer supported his claim. I absolutely do not believe that these marks are due to a hot lamp, for multiple reasons.
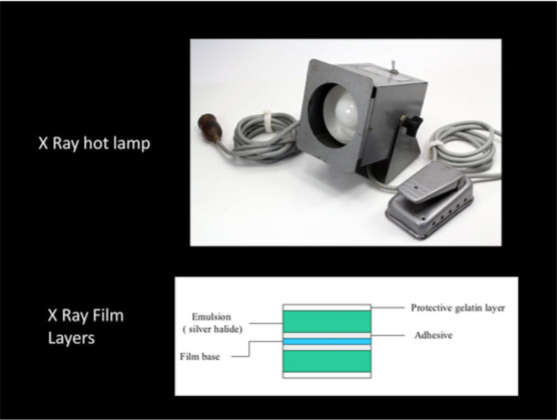
This is a typical “hot lamp” or hot light used to view dim areas of an x-ray. X-ray film layers are demonstrated in the lower image.
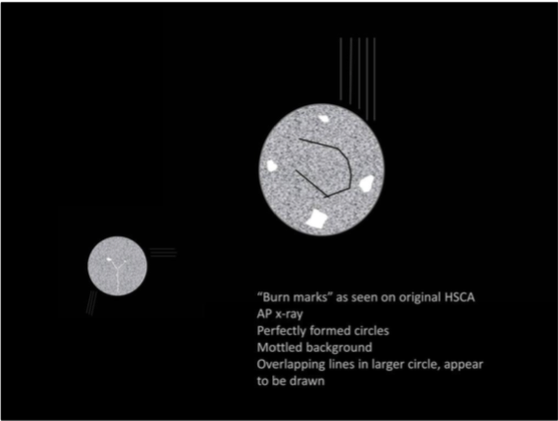
This is the appearance of these same areas as I saw them on the actual HSCA computer enhanced x-rays. I still don’t know what to make of much of what I’m seeing in these marks. On the HSCA film and on the original AP film, these are perfectly round. At the edge of both circles I could see the layers of the film clearly outlined. There was a mottled appearance of the background, and these intersecting lines in the larger circle. The white spots appeared the same as the metallic debris trail. The intersecting lines appear to be drawn onto the film – they are not due to any natural phenomenon or film processing.
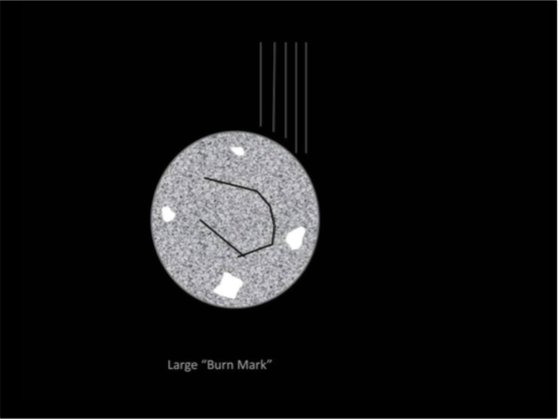
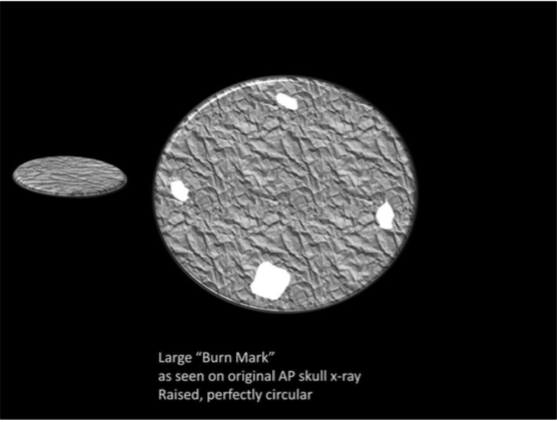
This is the appearance of the large burn mark on the original AP film. Perfectly round, with metallic appearing densities inside, and the surface was raised and crinkled. I’ve talked with several radiologists who have seen burn marks on film, and none of them had ever seen a perfectly round mark made – they all described an irregular, crinkled area on the film. If I could view this film again, I would ask to take it out of the protective mylar covering, to look at the underside of the film, to compare the appearance of both sides of the film. The circle appeared raised off the surface.

Again, perfectly round, with concentric margins at the edge.
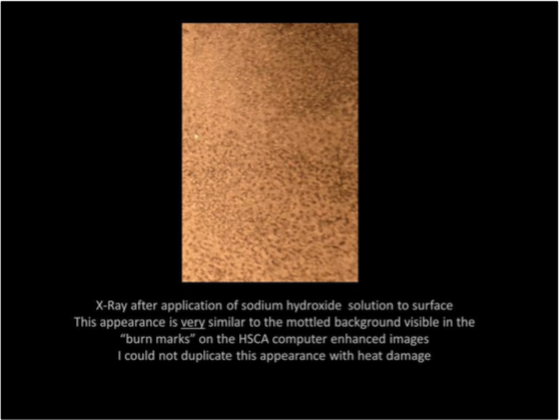
I tried to duplicate a burn mark on x-ray film from the 70’s and I couldn’t do it – it would burn straight through, and the edges simply turned brown. I stumbled onto this, thinking that whoever made these marks may have tried to use a chemical to dissolve the silver in the film. Sodium hydroxide can be used to recover silver from x- ray film and this is a close-up photo of a film treated with NaOH.
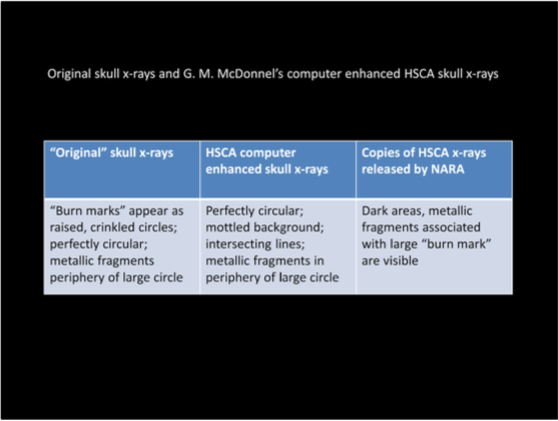
This is a comparison of the original films, the HSCA computer enhanced images, and then the copies of the HSCA images released to the public.
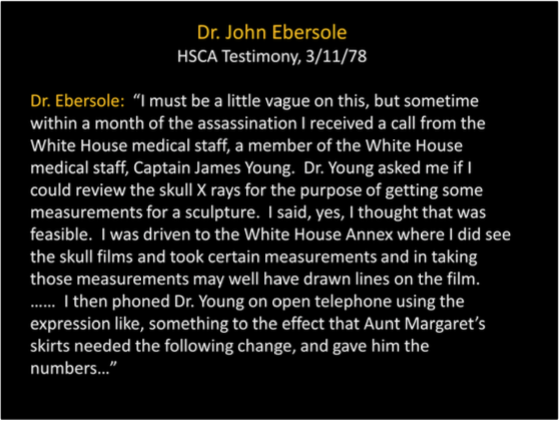
Now back to Dr. Ebersole – who took the fall for the “burn marks” This tall tale is included in his HSCA testimony. It’s an incredible story – Dr. Young was never called to testify. Could it have something to do with the burn marks, or the white patch, or the 6.5 mm object? I don’t know. I think that it is safe to conclude that the x-ray of the fractured, deformed skull was not used to prepare a bust of the President. I don’t presume to know if Dr. Ebersole made some of the alterations to these films, or was ordered to take the blame, however I think that the latter is more likely.

I’d like to give you a little background information on Dr. McDonnel, since he produced the computer enhanced images of the x-rays for the HSCA.
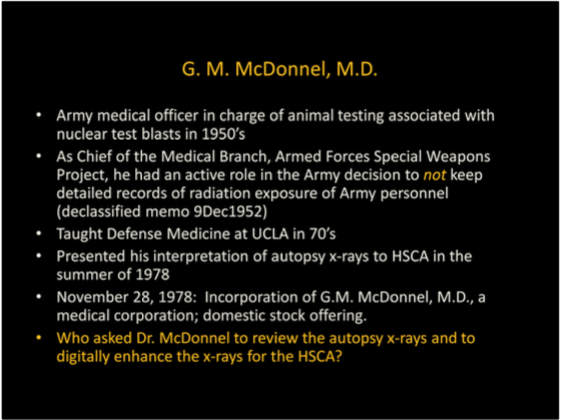
I stumbled across this insurance advertisement from 1963, featuring Dr. McDonnel – he had left active duty by this time.
This is from Dr. McDonnel’s report to the HSCA dated August, 1978.
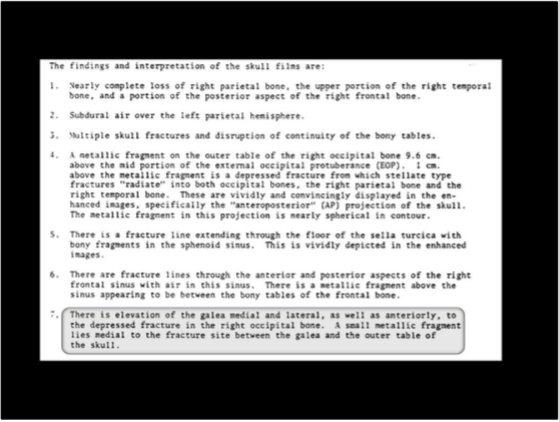
He described the fragment in occipital region as lying between the skull and the galea. He said that this fragment bounced back from the bone, to be embedded between the bone and the galea.
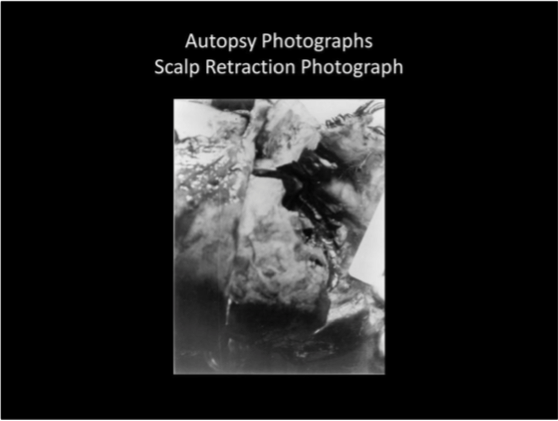
Next I’d like to present a brief review of the cranial photographs, beginning with the scalp retraction photograph. James Fox was a photographer with the intelligence division of the Secret Service, and he kept some of the autopsy photographs for himself. He sold them in 1981. Maybe this was legal – but to me it clearly violates the spirit of the Deed of Gift. In addition, these images are cropped and are not as clear as the originals.